What Is Interventional Cardiology?
A man in the throes of a heart attack arrives at the emergency room worried that he’ll need open heart surgery—and may even die. But what happens is nothing like what he expects.
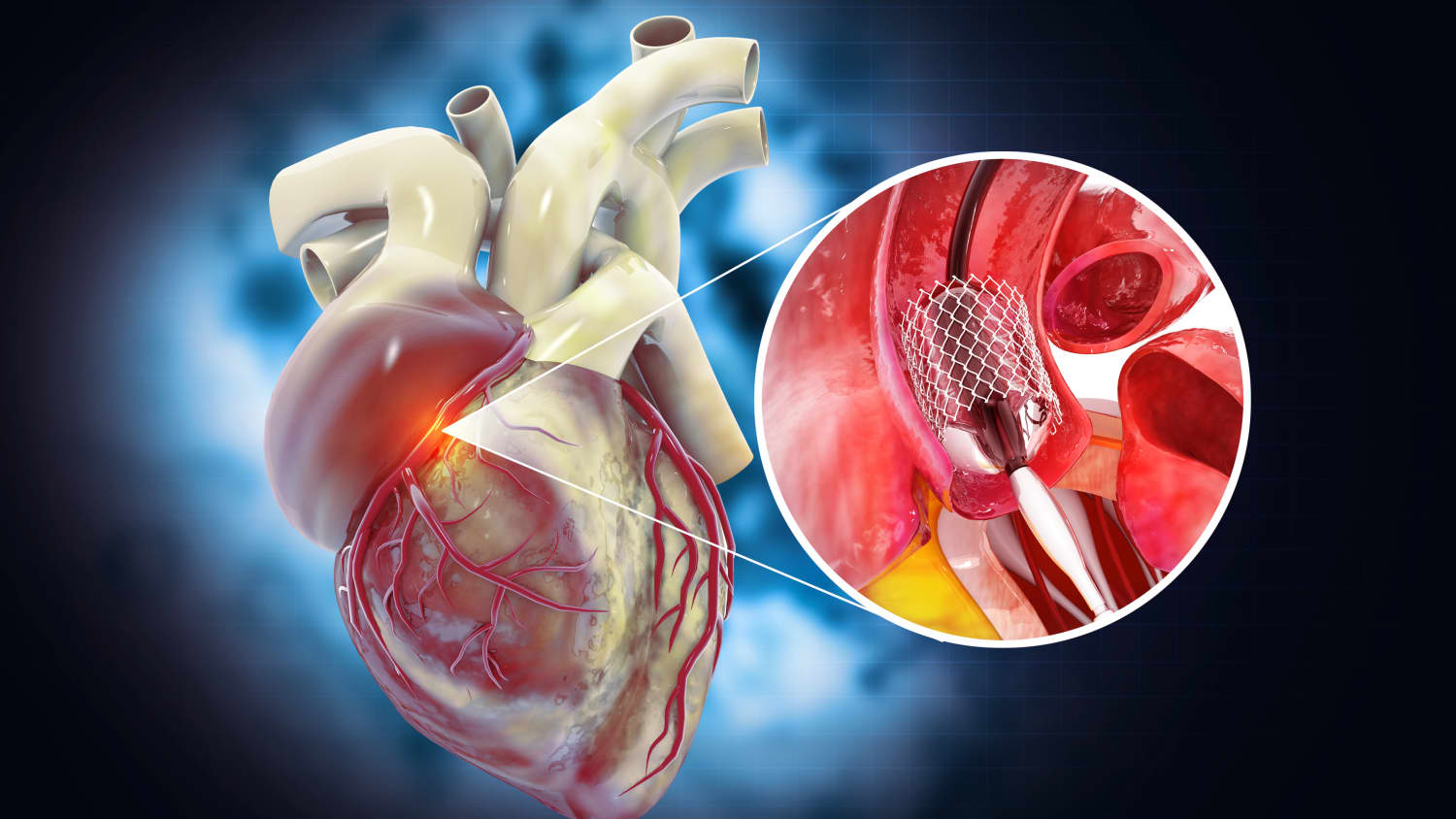
Doctors make a tiny incision in his groin and insert a catheter, a flexible tube thin enough to thread up through an artery toward his heart, where it delivers a tiny mesh coil called a stent. This opens the blocked artery, blood flows normally again, and his chest pain vanishes. He’s awake the whole time and goes home the next day.
This is interventional cardiology—a revolutionary field that uses catheter-based procedures to treat heart conditions, from plaque-stuffed arteries to aortic aneurysms, without major surgery. Relief from chest pain, fatigue, and shortness of breath is often immediate—and the outcomes can be life-saving.
“Interventional cardiology is one of the most exciting evolutions in heart disease,” says Yale Medicine specialist John K. Forrest, MD, director of interventional cardiology and the structural heart programs for the Yale New Haven Heart and Vascular Center and Yale New Haven Health System. “Fifteen years ago, the field was primarily focused around coronary interventions. However, the past decade has seen an expansion of the field—in addition to treating coronary disease, we now are able to treat valvular and other structural heart diseases through a minimally invasive approach.”
A new era of heart care
Interventional cardiology has always been a lifesaving procedure for people having a heart attack. With new technologies and therapies, the field is now able to positively impact the lives of many patients, offering them an alternative to open heart surgery.
Catheter-based procedures aren’t used for every heart condition or every person—such factors as a complicated anatomy can make navigating a catheter to the heart too difficult—and traditional open surgery is still the preferred approach for certain heart conditions. But interventional cardiology has been marked by groundbreaking advances, and the development of new devices and techniques. Research studies have shown some procedures to be as good or better than surgery.
How are interventional cardiologists different than general heart specialists—and why would you be treated by one?
Interventional cardiologists are heart specialists with advanced training in minimally invasive, catheter-based procedures. After completing medical school and a general internal medicine residency, they go through a three-year general cardiovascular disease fellowship and a one-year interventional cardiology fellowship. Some choose to pursue further specialization, especially in areas like structural heart disease, peripheral vascular interventions, or complex high risk interventional procedures (CHIP).
In addition to coronary artery disease and heart valve disorders, these specialists are trained to treat conditions such as atrial fibrillation, congenital heart defects, peripheral artery disease, and heart failure. They may be skilled in certain techniques; for instance, angioplasty, in which a small balloon is guided through a catheter up to the heart, where it is then expanded to widen a vessel that has narrowed—often as a result of plaque buildup from cholesterol, peripheral artery disease (PAD), or type 2 diabetes.
When do I need to see an interventional cardiologist?
You could be referred to an interventional cardiologist—regardless of your age and health status—if you have symptoms such as chest pain, shortness of breath, or fatigue; have been diagnosed with a heart condition that may require a stent or valve replacement; or are seeking an alternative to traditional open heart surgery.
Initially, catheter-based approaches targeted only people considered high risk for complications from open heart surgery, often due to age or other health conditions. But as techniques improved, people who are otherwise healthy and are at low-risk are now candidates for these procedures.
“We realized that if these approaches worked so well in high-risk patients, they should be available to others too,” Dr. Forrest says. “Over the last decade, doctors at Yale have participated in and led a number of national studies looking at this.” Some of the Yale studies focused on transcatheter aortic valve replacement (TAVR), a catheter-based procedure used to treat a narrowed aortic valve. In 2019, the Food and Drug Administration (FDA) expanded its approval for TAVR to patients regardless of their open heart surgery risk.
How is an interventional cardiology procedure performed?
While a heart attack demands immediate care, many catheter-based procedures are less urgent and performed on an outpatient basis. As opposed to open heart surgery, which requires a stay in the intensive care unit and possibly up to a week in the hospital, patients who undergo a transcatheter approach are usually discharged the next day.
These procedures use real-time imaging (ultrasound and fluoroscopy) to guide a thin, flexible catheter through a small incision, usually in the groin or wrist. “The femoral artery in the groin is one of the largest arteries in the body, and through it we can insert a fairly large catheter and deliver a variety of devices,” Dr. Forrest says.
When a heart valve is failing, doctors can use a catheter to deliver a synthetic replacement valve that is “crimped on a balloon” so it fits inside a blood vessel. Once it reaches the site of the failing valve—a one-way “door” in the vascular system that controls blood flow—the balloon and new valve are expanded, replacing the defective valve and restoring normal blood flow.
What are some common catheter-based procedures?
Three common examples of catheter-based procedures include:
- Angioplasty for atherosclerosis: This procedure is a crucial treatment for heart attack and may also be performed on a non-urgent basis to open coronary arteries that are narrowed or blocked, often by atherosclerosis, a buildup of cholesterol, fatty substances, and other debris known as plaque. It utilizes a catheter with a tip holding a balloon that can be inflated to push the plaque against the wall of the artery. A stent may be placed to keep the artery open.
- Transcatheter aortic valve replacement (TAVR): This is now the predominant treatment for aortic stenosis—more common than surgical aortic valve replacement (SAVR). Aortic stenosis is a narrowing of the heart’s aortic valve (the one that regulates blood flow from the heart’s main pumping chamber into the main artery of the body). With TAVR, the patient is sedated but awake while a surgeon and interventional cardiologist maneuver a catheter to the heart to deliver a replacement valve.
- Endovascular aneurysm repair (EVAR) for abdominal aortic aneurysm: This is a catheter-based approach to treating an abnormal bulge that can develop anywhere on the aorta, the main artery in the body. If a bulge ruptures, it can be life-threatening. But if the condition is caught early enough, EVAR is a treatment that involves making small incisions or punctures in the groin and inserting a catheter to place a stent that reinforces the weakened section of the aorta.
Other interventional procedures available at Yale Medicine include diagnostic cardiac catheterization, blood flow support for people who have received a heart transplant, and brachytherapy (a type of radiation therapy) for coronary artery stenosis.
How are these techniques changing the experience of people with heart problems?
Open heart surgery is still the best treatment in some situations, says Dr. Forrest. But it takes a toll on the body, he adds. For one thing, open heart surgery is very invasive. It may involve opening the chest cavity and connecting the patient to a heart–lung machine to temporarily stop the heart and take over its function. “Historically, about 50% of patients who needed to have a heart valve replaced never had it done because of the risks,” Dr. Forrest says.
People who have catheter-based procedures recover much more quickly than they would from traditional surgery. Often, they are quickly back to activities such as hiking and working outdoors, Dr. Forrest says. “In fact, we see this with younger and younger patients, including athletes, or people who work as firefighters or police officers who would have needed to take months off after surgery and worried about how that would affect their lives.”
In addition, data is accumulating to show that interventional procedures are effective—at least as good as open heart surgery, and in some cases better, Dr. Forrest says.
Dr. Forrest describes a randomized Yale study in which 800 patients were assigned to have open aortic valve surgery, and the other 800 were assigned to have TAVR. “We observed that the patients who had TAVR spent less time in the hospital and recovered more quickly than those who had traditional surgery,” he says. “Now we've been following those patients for five years. Overall, the two groups are both doing well."
How do you see interventional cardiology evolving?
Interventional cardiology is evolving rapidly thanks to innovations in advanced imaging, artificial intelligence, and new device designs, according to Dr. Forrest. New tools are making procedures safer, more precise, and accessible to more people. Examples include drug-coated balloons that can help prevent arteries from narrowing again, and next-generation stents that are designed to reduce inflammation and improve healing.
But this evolution has been happening for a while, he adds. For people who have peripheral arterial disease, “the catheters we use in the leg are much smaller today than they were even 10 years ago,” he says. Smaller catheters mean less discomfort and fewer vascular complications, and the ability to treat a wide variety of people. “Because patients have arteries in their legs of varying sizes, we can treat more people with a catheter-based approach.”
One of the biggest breakthroughs is in treating a “leaky” tricuspid valve (which directs blood flow on the right side of the heart). For years, it had so few treatment options that doctors called it “the forgotten valve.” That changed in 2024, when the FDA approved the TriClip G4™, a catheter-placed clip that brings together the tricuspid valve’s leaflets, which can reduce the blood leakage. A similar device called the MitraClip™ is available for the mitral valve, located on the heart’s left side.
Yet another improvement has been around for years: Makers of replacement heart valves have been using a special metal called nitinol, a combination of nickel and titanium. Originally developed by NASA, nitinol can be compressed for delivery through a catheter, then expand to its full shape once inside the warm environment of the body. “When nitinol is cold, you can form it into whatever shape you want, including the shape of a heart valve,” Dr. Forrest says.
How can a person find out if they are eligible for an interventional cardiology procedure?
Dr. Forrest advises anyone who is seeking treatment for heart disease to seek care at a comprehensive valve center where cardiologists, interventional cardiologists, and other specialists work together as a team and perform a high volume of procedures, provide different treatment options, and are involved in clinical trials that could lead to further improvements in care.
“There's nothing better than seeing a patient say, ‘I can now go out and do what I want to do and my shortness of breath and suffering is gone,’” Dr. Forrest says. “I recently treated a 90-year-old woman, who later sent me a postcard with a picture of herself carrying her kayak down to the ocean. She said (with a smile), ‘I am back on the water again. I used to kayak every day three years ago, but had to stop because I was so short of breath. I'm now back to doing it, and this is what I live for!’”

